Understanding Motion Sickness: The Neurological Science and Practical Remedies
For many, the excitement of a long-distance road trip, a scenic flight, or a cruise is heavily overshadowed by the dread of motion sickness (clinically known as kinetosis). It is a condition that can transform a premium travel experience into a state of physical distress.
Interestingly, a distinct paradox exists: the individual behind the steering wheel almost never suffers from this ailment, while passengers—especially those relegated to the rear seats—are highly susceptible. This article delivers a comprehensive, analytical look at the physiological mechanisms that trigger travel nausea and provides a structural blueprint to prevent and mitigate its symptoms.
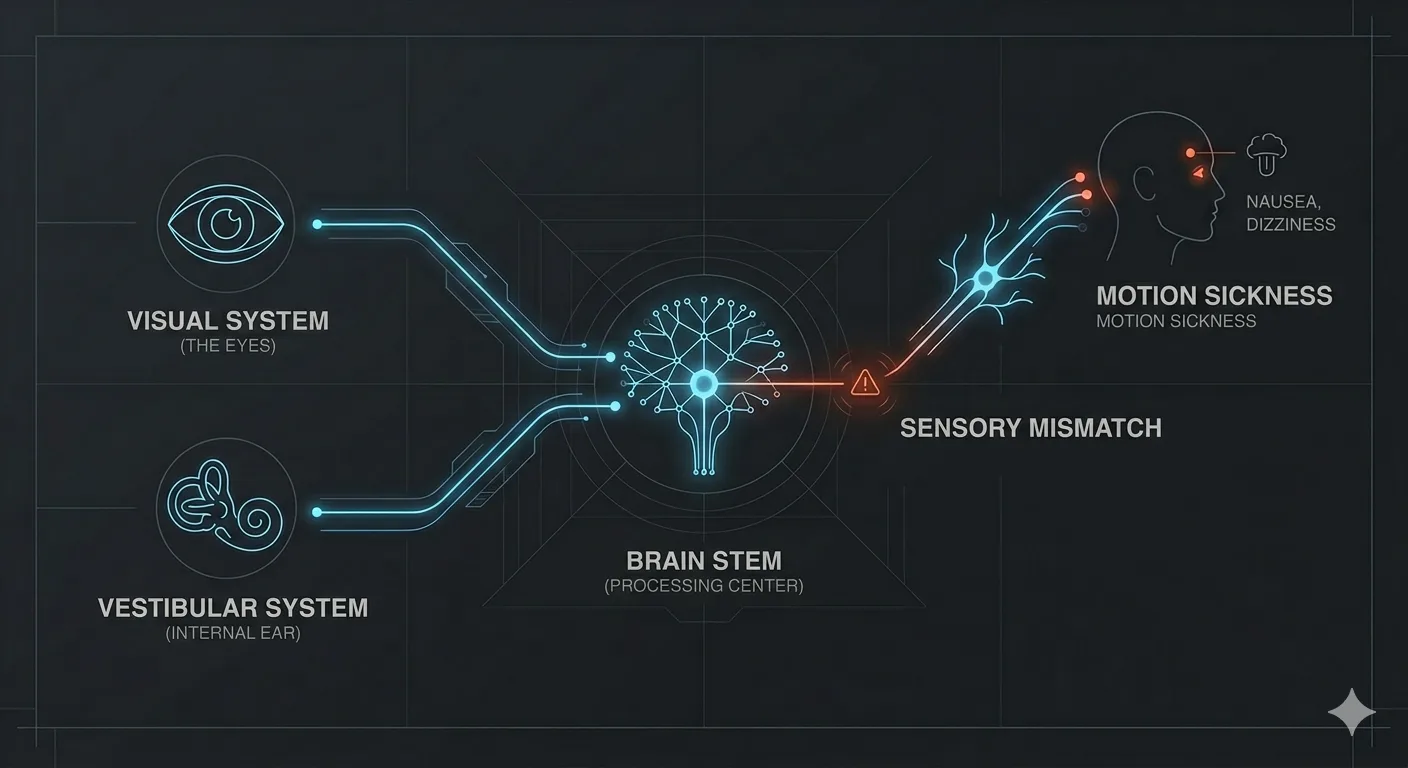
[Visual Subsystem] ---------> (Eyes view static interior) ---
[Vestibular Subsystem] -----> (Inner ear detects movement) ---> [BRAIN STEM] ---> Sensory Mismatch ---> Nausea/Vomiting
/ (Hypothalamus) (Defensive Alert)
[Proprioceptive System] ----> (Muscles detect G-forces) ----/
The Core Mechanism: Sensory Conflict Theory
Motion sickness is not a disease of the stomach; it is a functional mismatch within the central nervous system. To maintain equilibrium and navigate spatial orientation, the human brain continuously aggregates and cross-references data from three distinct physiological pathways:
-
The Visual System: Your eyes, which map your position relative to your immediate surroundings.
-
The Vestibular System: The intricate, fluid-filled semicircular canals within the inner ear that act as a biological accelerometer, detecting gravity, rotation, and linear motion.
-
The Proprioceptive System: Sensory receptors embedded in your muscles, tendons, and joints that report physical posture and the mechanical forces acting upon your body.
Kinetosis is triggered when these three subsystems transmit incompatible data streams to the brain stem.
The Classic Passenger Scenario
When a passenger reads a book or scrolls through a smartphone in a moving vehicle, their eyes remain locked onto a static object. The visual system sends a clear signal: the body is stationary. Concurrently, the fluid inside the vestibular system sloshes with every acceleration, braking maneuver, and corner, sending an opposing signal: the body is moving at speed.
This neurological dissonance causes the brain to experience a processing error.
⚠️ Evolutionary Note: The prevailing evolutionary hypothesis suggests that the brain interprets this profound sensory mismatch as the ingestion of a neurotoxin. Because hallucinogenic poisons disrupt sensory coordination in an identical manner, the organism initiates a primitive defense mechanism: activating the emetic center (the vomiting reflex) to purge the suspected toxin.
Technical Comparison: Spatial Inputs Across Different Cabin Roles
The severity of kinetosis depends heavily on an individual’s role and positioning within the vehicle. The table below breaks down how different seating positions alter sensory input and affect susceptibility.
| Vehicle Role / Position | Visual Input Status | Vestibular Input Status | Proprioceptive Input Status | Susceptibility Level |
| Driver | Dynamic & Predictive (High focus on distant horizon) | Synchronized (Anticipates acceleration/G-forces) | Active engagement (Hands on wheel, feet on pedals) | Extremely Low |
| Front Passenger | Dynamic & Reactive (Clear view through windshield) | Unsynchronized (Reacts after the movement occurs) | Passive resistance (Supported by seat/dashboard) | Moderate |
| Rear Passenger (Side) | Mismatched (Perceives fast-moving peripheral scenery) | High Impact (Subject to enhanced vehicle sway/roll) | Passive (Prone to lateral displacement) | High |
| Rear Passenger (Center) | Semi-Dynamic (View forward between front seats) | Balanced (Positioned on the vehicle’s central axis) | Passive (Minimal lateral stabilization) | Moderate to High |
Why Drivers Are Immune: The Motor Feedback Loop
The reason drivers remain unaffected by motion sickness lies in a neurological mechanism called the efference copy or the motor feedback loop.
When a driver decides to navigate a sharp curve, the brain issues a motor command to turn the steering wheel and flex the neck muscles. Simultaneously, the brain sends an internal duplicate of this command directly to the vestibular system. The inner ear is warned a fraction of a second before the physical movement occurs.
Because the brain accurately predicts the ensuing G-forces, there is zero sensory surprise. The passenger, conversely, can only react to the motion after it has commenced, leaving their vestibular system perpetually caught off guard.
Clinical Symptoms: The Progression of Kinetosis
Kinetosis does not manifest instantly; it follows a predictable physiological escalation. Recognizing the early, subtle markers allows for early intervention before the emetic reflex becomes irreversible.
Phase 1: Physiological Prodrome
-
Frequent Yawning: An involuntary neurological response to early cerebral disorientation.
-
Slight Drowsiness: The brain attempts to suppress the chaotic sensory inputs by inducing lethargy.
-
Paloare (Facial Pallor): Vasoconstriction shifts blood flow away from the skin surface.
Phase 2: Active Distress
-
Cold Sweats: Sudden activation of the sympathetic nervous system, localized on the forehead and palms.
-
Hyperventilation: Rapid, shallow breathing as the autonomic nervous system destabilizes.
-
Sialorrhea: Excess salivation, which naturally protects tooth enamel from gastric acid prior to emesis.
Phase 3: Crisis
-
Severe Vertigo: A complete loss of spatial orientation.
-
Nausea and Emesis: The final activation of the gastric motor program.
Evidence-Based Solutions and Practical Mitigations
Managing motion sickness requires a systematic approach aimed at reducing sensory conflict, stabilizing physical anatomy, and optimizing the cabin environment.
Behavioral Modifications for Passengers
-
Establish a Distant Visual Reference: Look straight ahead through the front parbriz. Fixate your eyes on the distant, stable horizon line rather than neighboring vehicles. This provides the visual cortex with a geometric anchor that matches the velocity data from the inner ear.
-
Anatomical Stabilization: Firmly press your head back against the headrest. Minimizing the micro-movements of the skull reduces the chaotic fluid dynamics within the semicircular canals.
-
Utilize the Structural Grab Handle: Holding the overhead safety handle allows your muscular framework to establish a rigid point of counter-leverage, helping your proprioceptors register vehicle roll more accurately.
-
Optimize Ventilation: Direct cool, moving air from the HVAC vents directly onto your face. Lowering ambient temperature and maximizing fresh oxygen delivery actively suppresses the activation of the brain’s nausea centers. Avoid strong cabin deodorizers, perfumes, or tobacco smoke.
-
Visual Elimination: If symptoms become unmanageable and the vehicle cannot stop, close your eyes completely. By eliminating the false visual data stream, the brain defaults exclusively to the vestibular inputs, resolving the primary conflict.
Pharmacological and Natural Interventions
When behavioral adjustments prove insufficient, targeted biochemical options can prevent or arrest the symptoms of kinetosis.
Natural Gastric Regulators
-
Zingiber Officinale (Ginger): Clinical studies demonstrate that ginger contains active gingerols and shogaols that act locally on the gastrointestinal tract. It modulates antral contractions and delays the development of gastric dysrhythmias, effectively neutralizing nausea without affecting the central nervous system. It should be consumed 30 minutes prior to departure via capsules or concentrated extracts.
-
Peppermint Aromatherapy: Inhaling high-purity essential oil of peppermint provides a cooling sensation that stimulates the trigeminal nerve, serving as a powerful sensory distraction that dampens the perception of visceral distress.
Clinical Modulators
-
Antihistamines: First-generation H1 receptor antagonists (such as dimenhydrinate or meclizine) cross the blood-brain barrier to depress vestibular excitability and inhibit neural pathways in the vestibular nucleus. Due to their sedative side effects, they are highly effective for passengers but must never be consumed by the driver.
-
Anticholinergic Agents: Scopolamine patches, applied to the post-auricular mastoid region several hours before travel, transdermally deliver a steady dose that blocks muscarinic receptors in the vestibular apparatus, offering prolonged protection for long-distance maritime or overland travel.
Verdict and Final Strategy
Motion sickness is a physiological design limitation of the human brain, born from a sensory contradiction between what we see and what we feel. It can be systematically managed.
To guarantee a symptom-free journey, passengers should claim the front seat, strictly avoid digital screens, maintain a fixed gaze on the horizon, and preemptively deploy natural or over-the-counter vestibular suppressants at least half an hour before the vehicle begins to move.
✍️ Author: Bejenaru Alexandru Ionut – [email protected]
🔗 Internal link: https://diagnozabam.ro/sfaturi
Searching for a rugged, handheld scanner covering the 4 vital systems with worldwide vehicle coverage?

Looking for a complete all-system diagnostic tablet that is stable and built for daily multi-brand workshop use?
